
Common Cerebral Palsy Therapies and Specialists

Although every individual with cerebral palsy has unique support needs, there are some common concerns for families to be aware of. Here are the top recommended therapies to support kids with cerebral palsy.
Who can be on your CP care team?
Each child’s care team is unique because every child’s needs vary. However, in general, pediatricians, pediatric neurologists, geneticists, pediatric rehabilitation physicians, and developmental behavioral specialists can diagnose and treat cerebral palsy (CP).
Dr. Andrew Collins, a pediatric rehabilitation medicine physician at Stanford Medicine Children’s Health, says it’s important for parents to come up with goals and to work together with their care team to determine what is a good way to set goals that meet their child’s medical needs while thinking about what that individual enjoys and what that family values. He says, “I think the desire to engage families in those goals should be a supportive desire to engage families, not one where we abandon the family and expect them to make all of those decisions on their own, but to really just engage them in what areas are priorities for them and help support for coming up with goals that are really helpful and can work together to help a kid get there.” Once CP has been diagnosed, a variety of specialists can help with any co-occurring conditions that might also occur.
- Developmental pediatrician
- Ear, nose, and throat doctor (ENT)
- Endocrinologist
- Epileptologist
- Neurogeneticist
- Neuro-ophthalmologist
- Nutritionist
- Occupational therapist
- Optometrist
- Orthopedist
- Pediatric audiologist
- Pediatric gastroenterologist (GI)
- Pediatric neurologist
- Pediatric ophthalmologist
- Pediatric physiatrist
- Physical therapist
- Psychologist and/or psychiatrist
- Clinical child psychologist
- Developmental psychologist
- Educational psychologist
- Pediatric neuropsychologist
- Pediatric psychiatrist
- Speech therapist
- Vision therapist
Build my child's care team
Physical therapy
Dr. Collins tells Undivided the various things he and physical therapists can do to help children with CP maneuver around their home and communities with greater ease. He says they work together with other specialists to help individuals find the right therapies and medications and they support people with CP in all the things they want and need to do, especially for those who have trouble doing them regularly.
Pediatric rehabilitation medicine doctors work with children with cerebral palsy to monitor their overall medical trajectory such as making sure they’re getting effective treatments, having the right adaptive equipment, monitoring ways braces may help, and managing the symptoms they might be having like spasticity or other forms of hypertonia. These doctors also recommend medications or procedures that help with pain and discomfort as well.
For example, in some cases, surgery may be needed to correct orthopedic issues. Dr. Lekha Rao, an associate professor of pediatric neurology at UCLA’s David Geffen School of Medicine says that tendon-release surgery is an option that can help elongate muscles. Surgery to cut nerve fibers is another. Research and clinical trials are underway for stem cell therapy, which have been used for regenerative purposes, but is still new for CP.
In this clip, Dr. Collins explains specifically what physical therapists do to help children with CP navigate the world:
PT also uses various adaptive equipment depending on what they need help with. Dr. Collins says PTs might use what the kids have at home, such as a walker, gait trainer, or their braces. Sometimes, PTs use an electrical stimulator device to help activate or contract a muscle when an individual is unable to perform that on their own. On other occasions, PTs provide bodyweight assistance like a lift overhead or robotic device to help with walking on a treadmill. These training sessions are beneficial for someone who is learning to walk and needs to get more steps in or those who are unable to provide “all the body weight themselves,” he says. Sometimes, physical therapists will use a stander to help individuals with CP stand upright to help get weight through their legs to support bone development and strength in their legs and core.
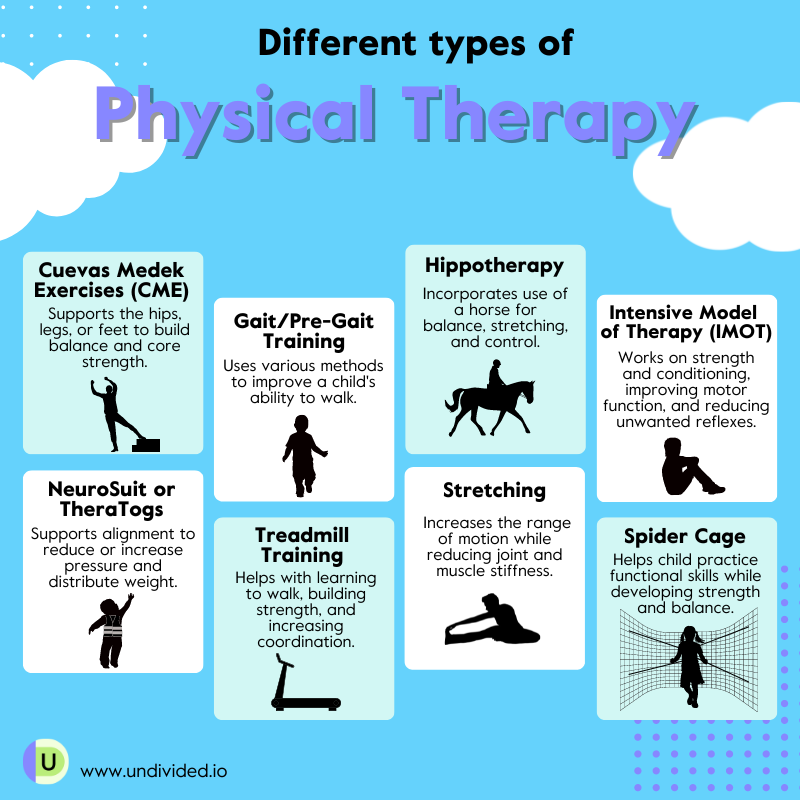
Another therapy you might have heard of is a spider system, which is a form of physical therapy treatment that keeps someone in an upright position. Dr. Collins says, “Those supports can be used together with a treadmill, for example, to help with gait training, or treadmill training, for walking, or they can be used in a variety of other ways to help with strengthening.” These types of help also support muscle retraining education.
“In the setting of different muscle tones, physical therapy will work on really appropriate positioning and strengthening and other things like that. In the setting of hypotonia, someone who has loose muscles, will want to work a lot on strengthening, maintaining good position of joints, maintaining good position in the environment, and functional activities. For someone with hypertonicity, which can often be spasticity or dystonia, which is a variable type of hypertonicity, we'll work on different strategies to reduce that tone. While we're also working on strengthening and good positioning in the setting of hypertonicity, we want to really work on a range of motion activities as well. We do that in hypotonia, too, but it's a little bit different in hypertonicity. The stretching that is done with a physical therapist, and the bracing the physical therapists can help with can often actually provide a treatment for that high level of tone and help to reduce the tone as well.”
Children with CP might need physical therapy throughout their lives. But the frequency varies. Dr. Collins says it’s beneficial to start kids with CP off early with therapies. "That's a good thing for children to be starting with early intervention therapies, being the therapies that happen between being born and age three, at least in the United States," Dr. Collins says. "Often that therapy can be pretty frequent and can often be like weekly therapies."
The kids may start with frequent physical therapy sessions in early childhood, but that often changes as they get older. Dr. Collins tells us, "That may move to a consultative physical therapy or physical therapy that people see a therapist a few times a year for check-ins, where they see how each of the joints are doing, if they're developing any issues with joints that are getting stuck, how they're doing with functioning, whether that's using their wheelchair walking around, going up and down stairs, and how each different areas are doing with muscle tightness. Then they'll either develop more of a home exercise plan to keep working on or they may do an intensive burst of therapy or an episode of care focused around a specific goal."
The important thing to remember is having a direct point of contact with a physical therapist who knows the child well will go a long way in facilitating improvements.
Dr. Collins further adds, “Whether that's newly being able to help with specific types of transfers to get from say, their back chair to their wheelchair, or whether that's practicing swinging a bat to joining the high school baseball team. In the setting of weakness in one of their arms and they want to get stronger, anything like that can be done together with a physical therapist. And it's really helpful if it's one that knows you a little bit.”
Physical therapy doesn’t have to be all hard work. Your child can have a lot of fun, too! Depending on their functional levels, adaptive bikes are a great way for kids to cycle, increase their movements, and exercise. Adaptive bikes have three wheels to provide stability for the rider, and they can be customized to fit anyone from toddlers to adults.
Dr. Collins says, “Even for those who aren't pedaling, the act of maintaining an upright posture on a cycling device, whatever type that is, could also give them some exercise related benefits related to that trunk control or the balance. And even if someone's not pedaling, but they're participating in a cycling event, that's also really good in terms of participating in recreational activity and engaging with the community.”
For those with limited leg mobility, handcycles are a good option and use hand cranks in place of pedals. Adaptive stationary, tandem, and recumbent bikes can also be fun and help with heart health and improve muscle function.
For children with CP who are too young or for other reasons unable to use an adaptive bike, there are strollers and pushchairs that allow them to go to places and participate with their families and friends in all manner of activities. Certain strollers can accommodate children and adults of all sizes, and they are also available with suitable all-terrain modifications. To learn more, read our article Physical Therapy (PT) 101.
Find a physical therapist (PT)
Occupational therapy
Occupational therapy (OT) helps with movement and functional issues. Occupational therapists use tools that promote mobility independence for individuals with physical, cognitive, and developmental disabilities. Amy Kim Luu, a pediatric occupational therapist at UCLA’s Outpatient Rehabilitation Services, shares how OT addresses the needs of children with CP. Luu works with kids of all ages, particularly from 0 to some young adults.
Some common functional issues that affect kids with CP in their day-to-day activities and skills are mobility and postural issues. Luu says, “We often see difficulties with posture and movement in children with CP. This can influence many functional issues, such as grasping (fine motor skills), sitting, standing, walking (gross motor skills), and oral skills to communicate and eat.”
As the name suggests, an OT works with an individual’s “occupations.” Luu explains what that looks like when she treats patients with CP. “As occupational therapists, we work with children of all ages with CP on their meaningful occupations. Occupations can include school, social participation, activities of daily living (bathing, grooming- brushing teeth, dressing), feeding, and most importantly, play. For example, working on sitting balance to reaching and grasping for their favorite toy. These occupations can change and grow across a child’s lifespan.” Luu says that can look anywhere from infant feeding to toddlers holding a spoon to self-feeding themselves. In feeding therapy, OTs teach kids with sensory and motor issues how to eat. They will create a plan to address obstacles your child might face in their ability to eat. Another challenge a child with CP faces is undiagnosed or underdiagnosed cortical visual impairment (CVI).

A typical OT session can vary, but an important part of the session is exploring a child’s interest and motivation and including that in their treatment plan, Luu says. Once that has been established, a session can look like this: “Having a child squat down to pick up their favorite cars on the mat and then standing to place the cars onto a race track on an elevated bench-[where] the child is working on strengthening, balance, coordination and intentional release while engaging in play. For another child with interest in cars, it could be positioning their body in side-lying on a mat to reach and push cars to race. Treatment varies for each child but the highlight is to have them participate and engage.” she says.
One of the goals of OT is to promote mobility independence. Luu tells us, “Occupational therapists are able to assess the initial level of where a child first starts on a task. Then, we are able to break down or adapt the tasks for increased participation and independence. An example could be dressing-a child with CP may initially require caregivers to complete most of the task to remove their socks. By providing strategies for positioning and breaking down the steps of removing socks into multiple, manageable steps, the child may now be able to increase participation (engaging in motor planning, strengthening, body awareness, and repetition of the task) to gain autonomy.”
OT doesn’t stop when the session ends in the outpatient setting. It continues at home, and family or caregiver engagement is critical in supporting individuals with CP to improve movement and function. “Education on positioning, hands-on manipulation, exercises and adaptive tools are provided in occupational therapy, however, therapy is only a few times a week or month,” Luu says. “A large component of therapy is the carry over and practice of home exercises. It can be as simple as engaging in more tummy time or taking the recommended strategies on positioning to facilitate and practice with equipment at home.”
To learn more, read our article Occupational Therapy (OT) 101.
Find an occupational therapist (OT)
Speech therapy
Many individuals with CP will also benefit from speech therapy. Teaching individuals with CP how to communicate and develop robust language skills is crucial to empowering them to have a fulfilling social and professional life. Many speech-language interventions can help, such as articulation therapy, oral motor or feeding and swallowing therapy, and augmentative & alternative communication therapy.
A speech-language pathologist will show a child how to make certain sounds in articulation therapy. They will demonstrate this using a mirror and show the child how to move the tongue to produce a sound. In feeding and swallowing therapy, oral exercises and massages are taught and applied to help strengthen the mouth muscles. A speech-language pathologist will also explore foods and temperatures to enable individuals with CP to increase their oral sense and awareness of eating and swallowing.
Ali Steers, owner of Steers AAC Language & Speech and a speech-language pathologist who specializes in Augmentative and Alternative Communication (AAC), tells us why individuals with complex bodies need language development and how communication can help them feel safe.
AAC support
While traditional speech therapy may be valuable for many people with CP, many can also benefit from AAC support — particularly if communicating through spoken language presents a significant challenge. Steers, who works with nonspeaking children, has seen many cases where kids communicate better after the introduction of AAC and addresses the myth that using an AAC device will hinder the development of spoken language.
Find an AAC specialist
Steers stresses getting a child evaluated by an AAC specialist as soon as a formal CP diagnosis has been determined. At a young age, children’s neural pathways are still forming, which makes it easier for them to learn a new method of communication like AAC.
AAC comes with a range of possibilities, from non-electronic to electronic systems. Non-electronic AAC can be an activity-specific display with key vocabulary for a particular activity such as reading a book, going to the bathroom or mealtimes. Electronic AAC systems can be a device, such as an iPad or dedicated communication device, with specific AAC software on it that a child can use to communicate. For individuals with CP whose motor difficulties make pressing buttons or pointing to pictures a challenge, AAC devices like the Eyegaze Edge and Tobii Dynavox TD I-Series allow children to use their eyes to select different pictures or icons or type out messages. And because many children with cerebral palsy also have cortical visual impairment, switch scanning methodologies for accessing electronic communication are often a viable access method as well.
One challenge that Steers mentions, though, is that many speech-language pathologists (SLPs) aren't trained in AAC. Many parents are also unaware of AAC, and not all school districts are well trained in how to implement it. Steers is also very mindful and aware when she’s working with individuals with CP that she’s not having the kids produce a movement that further challenges their motor system, especially because individuals with CP experience pain from some movements. “When I'm looking at access, I need to put those switches [for AAC] somewhere that's not going to result in or exacerbate pain for that person.” It's also essential to overcome our own biases and the longstanding myth that kids with CP cannot learn. Steers believe wholeheartedly that children with CP are communicators and can impact their world. Like any child, they just need adequate exposure to learning.
"Some children will learn something the first time that you present it, and some children will learn something the fortieth time you present it," Steers says. "That's just learning. And that's just all of our brains and how our brains are different.” However, it’s important to note that parents or caregivers need to be actively involved in supporting AAC usage to support kids in learning AAC. As with anything like learning an instrument or driving a car, it takes time and practice. AAC is like learning a new language. Expecting a child to learn AAC on their own won’t stick with them because it involves integration and immersion. The symbol language of AAC has to become a lifestyle for both the AAC user and their family.
Kids with CP can thrive alongside their peers
Steers brings up another interesting point about teaching communication skills to kids with CP. For someone with a complex body, the access methodology needs to be actively taught. “It’s not about finding access for them,” she says, “it’s about teaching it.”
In this clip, Steers discusses how kids with CP can learn like any typical peers. They just need opportunities to learn, and repetition is key. That, as we know, applies to adult learners as well.
Complementary therapies
Complementary and alternative therapies are often thought of as therapies that are considered outside of mainstream medicine," Dr. Collins says, "and the definitions of how we define what counts as part of mainstream medicine or not, it's kind of variable from person to person." He says each provider has a different way of defining that, and insurance companies, too. Insurance companies that designate a service as complementary or alternative may not cover them, so it's up to the families to decide and understand how those services are billed and whether it makes sense for them to have their kids engage in them at that moment.
Some lesser-known therapies that are helpful to kids with CP include:
- Aquatic therapy, where physical therapy is conducted in a pool, which can help build strength in a different setting and can support different muscles
- Horse-riding therapy, or hippotherapy, which helps with strength, posture, and balance
- Goal-oriented therapy, which Dr. Collins explains as "to do therapy around a specific goal and help someone achieve the goals that they're working on."
Dr. Collins provides examples of goal-oriented therapy. If someone wants to climb stairs using one hand on a handrail to get around school buildings from elementary to middle school because they have to go upstairs, the goal would be to do a session on that goal, specifically. That can “include strengthening their legs, working on balance, navigating the actual steps, using their hand for postural control, all of those different things are aspects of it,” he says. “And there may be various tools that are used to get there on that specific functional goal.”
Dr. Collins says, “Outside of physical therapy, in occupational therapy, for example, that also might include tying a shoe, or being able to stay in the upright position for someone to be able to feed you. So for some people, say, don't have great posture, so that they can swallow effectively and safely, would be a really good positioning goal that someone might work on in therapy too.”
He continues, "All of those kinds of sub-types of therapy, or specialized types, really go along together with the overall philosophy of doing goal-directed therapy to help people achieve the things that they want and need to achieve," Dr. Collins says. There are many complementary and alternative therapies aside from the above that your child might respond to, so consult with your child's care team to see what they recommend.
Common adaptive equipment for people with CP
Individuals living with CP often require adaptive equipment to get around and function with more independence. Sometimes known as Complex Rehabilitation Technology, this equipment could include a power wheelchair, stander, gait trainer, transport chair, adapted bike, forearm crutches, ankle braces, shoe orthotics, and more. These devices are medically necessary and are usually recommended by an occupational therapist, physical therapy, a doctor, or a rehabilitation technology professional.
Dr. Collins says, “Sometimes people will work with more specialized seating experts in physical or occupational therapy if they have a really complicated type of wheelchair that they're needing, or they need additional modifications to their wheelchair that are outside the scope of what their regular therapists are able to provide.”
Dr. Collins also tells us, “Some people with cerebral palsy may use different tools to do their activities of daily living or stuff that they do within their house. They may use a chair to help them maintain safe positioning in the bathroom or in the bathtub or shower, may use special chairs to stay safe in a car, might use other types of devices to help themselves do things like get dressed, fastened buttons.”
After the professional determines that adaptive equipment is needed, they will provide the prescription, documentation, and other support documents to submit to insurance for possible reimbursement.
Funding adaptive equipment
Leslie Lobel, Undivided’s Director of Health Plan Advocacy Services, tells us how to create a funding plan and understand the coverage and limitations of all available funding sources, so your child doesn’t get caught in a bind when the need for adaptive or intervention services arises.
“It’s important to identify all of your child's potential funders and to understand the order in which they will authorize payment,” Lobel says. “And also a more complex function is to understand what each funding source can and cannot do.” In short, if you have health insurance, you ask for medical support needs through the health plan, and if your child has educational needs, you request those supports from the school district, through your child's IEP.
Knowing what these funding sources can provide will help you cover your child's goals. It also saves time, energy, and headaches when you know which source to ask for what. For example, schools assist if a support helps the child meet their educational goals. Also, a school therapist typically works on different goals from what a private therapist does. A private physical therapist (PT), for example, might be concerned about your child walking or crawling posture because those are important parts of your child’s future overall physical development. A school PT, on the other hand, focuses on safety in the classroom, on the schoolyard, and on campus.
DME and low-incidence equipment
“Low-incidence funding is funding for equipment through the school district that's very specific for your child, or equipment that not many children need,” Lobel says. Low-incidence disability categories in special education include hard of hearing/Deaf, vision impairment, and orthopedic impairment. Lobel also says that you might have the same equipment at home funded through the health plan.
Lelah Coppedge recommends that you don’t prolong contacting the insurance regarding DME. Even if your child doesn’t need equipment now, they might later. The wait time to get an approval from insurance can be anywhere from 4 to 6 months or longer.
When your child has additional support needs due to a diagnosis like CP, it can be difficult to manage a team of therapists on your own. According to Lobel, "The family should consider the services of a specialized provider, such as a neurologist, a developmental pediatrician, or an orthopedist, depending on their child’s needs. Both to identify goals and interventions and to act as a case manager for coordinated care."
Fund durable medical equipment (DME)




Unlock more with Undivided
Turn knowledge into action that benefits your child
Get Membership




Author

