
Tourette Syndrome 101

Approximately 1.4 million people in the United States live with a chronic tic disorder, including Tourette syndrome — about 1 in every 40 people. The media often portrays Tourette syndrome as an irresistible urge to swear or say inappropriate phrases at random. This is, of course, not an accurate depiction; Tourette syndrome can look different for everyone. To help dispel common misconceptions, this article will walk you through what Tourette syndrome is, how it’s diagnosed, and how to support someone with Tourette syndrome at home and at school.
For expert insights to help us better understand Tourette syndrome, we spoke to John Piacentini, PhD, professor in the UCLA Department of Psychiatry and Biobehavioral Sciences and director of the UCLA Child OCD, Anxiety, and Tic Disorders Clinic; the Tourette Association Center of Excellence; and the UCLA Center for Child Anxiety Resilience, Education, and Support. We also spoke with Mary Peitso, non-attorney special education advocate, and Harper Word, a freshman in college who has Tourette syndrome.
What is Tourette syndrome?
According to Dr. Piacentini, Tourette syndrome is characterized by the presence of multiple motor tics and at least one vocal tic that have persisted for more than a year. Tics are sudden, involuntary movements or sounds that a person cannot simply stop on command. There has yet to be any identifiable reason why Tourette syndrome occurs.
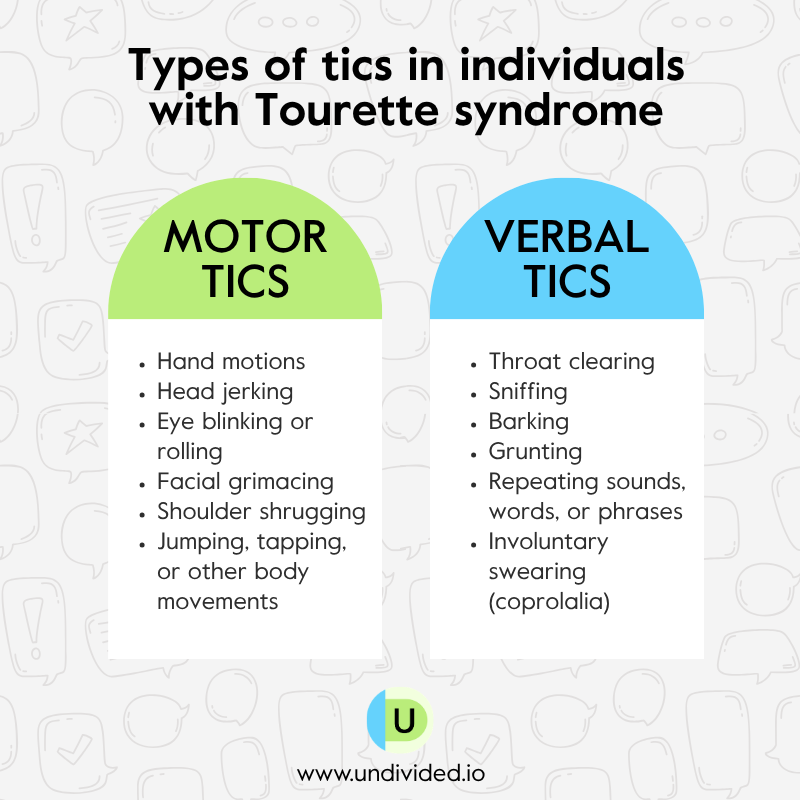
These symptoms generally fall into two categories: motor tics, which involve body movements such as hand motions, head jerking, or eye blinking, and vocal tics, which include sounds such as throat clearing, sniffing, or other repeated noises or vocalizations.
Types of tics
Motor tics:
- Hand motions
- Head jerking
- Eye blinking or rolling
- Facial grimacing
- Shoulder shrugging
- Jumping, tapping, or other body movements
Vocal tics
- Throat clearing
- Sniffing
- Barking
- Grunting
- Repeating sounds, words, or phrases
- In rare cases, involuntary swearing (coprolalia)
It’s easy to assume that if someone has a tic, they must have Tourette syndrome, but that is not the case. Having a single tic does not automatically mean a person has Tourette syndrome. To better understand the difference, we’ve broken down the three types of tic disorders.
The three types of tic disorders
1. Provisional tic disorder. Temporary motor or vocal tics that may be present for less than one year. In most cases, symptoms are short-term, with roughly 90% resolving within a year, sometimes after only a few weeks or months. Because many childhood tics are temporary, a formal chronic tic disorder diagnosis — such as persistent tic disorder or Tourette syndrome — typically requires tics to be present for more than one year.
2. Persistent (chronic) motor or vocal tic disorder. Tics that have been present for more than one year but involve either motor tics or vocal tics, but not both. Persistent motor tic disorder is more common than persistent vocal tic disorder.
3. Tourette syndrome. Both multiple motor tics and at least one vocal tic have been present at some point for more than one year, although symptoms may ebb and flow over time. The onset of this disorder usually starts between the ages of 5 and 7 years old.
In this video, Piacentini dives deeper into the three classes of tics:
Functional neurological disorder (FND) with tic-like behaviors
Provisional tic disorder, persistent motor or vocal tic disorder, and Tourette syndrome are the three types of tic disorders. However, in recent years, there has been a rising incidence of functional neurological disorder (FND) with tic-like behaviors. According to the Tourette Association of America, FND with tic-like behaviors shares many features with other tic disorders, but the main difference is that FND occurs in young adults — particularly females — ages 17+ who have had no prior history of any tic-like behaviors.
One key difference between tic disorders and FND with tic-like behaviors is that many tic disorders usually begin gradually in early childhood and often start with simple motor tics, such as blinking or facial movements. FND with tic-like behaviors, on the other hand, more often appears suddenly in teens and young adults who did not previously have a history of tics. Symptoms may be more intense at onset and can involve larger, more complex movements or vocalizations.
Experts believe the increase may be connected to higher levels of stress, anxiety, and mood challenges during and after the COVID-19 pandemic. FND with tic-like behaviors is also commonly seen alongside conditions such as anxiety, depression, or obsessive-compulsive disorder.
The most important thing for parents to know is that these symptoms are real, and children are not faking them or doing them on purpose. Because tic disorders and FND can look similar, it’s helpful to work with a health care provider who understands both so your child can get the right support.
What do tics feel like?
According to Harper Word, a freshman in college who has Tourette syndrome, tics can feel like a pressure that gradually builds and can only be relieved once the tic happens. This urge is commonly known as a premonitory sensation and is commonly described as an urge, tension, pressure, and/or itching that becomes increasingly uncomfortable until the tic is released.
Dr. Piacentini elaborates on why that urge/sensation is so powerful. When a tic happens, the uncomfortable sensation goes away, and that relief reinforces the behavior.
“The tic is designed to make a bad feeling go away, and it works really well,” he explains. “It’s like every time I say thank you, I get a nickel. I’m going to be saying thank you to everybody.”
In other words, the tic is rewarded by the relief it brings, which is part of why it persists. That said, Dr. Piacentini notes that it isn’t quite that simple, as tics have a life of their own beyond just responding to premonitory urges.
He also describes Tourette syndrome as a disorder of inhibition. Dr. Piacentini explains it as the brain having difficulty stopping unwanted movements or sounds, like a filter with leaks that let certain signals through as tics. When someone feels pressure to suppress a tic, particularly in a stressful setting, they tend to focus on it more and, therefore, express more tics.
What age do tics show up?
The average onset for tics is usually around 5–7 years old. While this is the average age of onset, it does not apply to every child. Dr. Piacentini notes that some children experience tics nearly from birth or as early as age 3–4, while others may not have symptoms emerge until age 8–9.
In cases where tics begin later in childhood, clinicians often look back at earlier history. Because some tics can be very subtle, parents may not notice symptoms that have been present for some time. Dr. Piacentini explains that some teenagers come in having never been diagnosed, and when asked, the child may reveal they had tics when they were younger but worked to suppress or hide them.
How Tourette syndrome is diagnosed
For Word, the path to a diagnosis wasn’t as straightforward as it is for some. She first noticed tics becoming a significant part of her life around seventh or eighth grade, but it took months of uncertainty (and worrying) before anyone could explain what or why it was happening. “It took a long time to realize that something medical was going on and I wasn’t just an odd child,” she says. Getting a formal diagnosis brought its own kind of relief.
“Realizing that I wasn’t the only one in the world doing this was such a comfort. Being able to go to the doctor and definitively say this is what’s causing this, and this is how we can manage it — that was really nice."
Dr. Piacentini says the process of getting a formal Tourette syndrome diagnosis typically starts with a pediatrician, who may then refer families to a specialist. When a child comes in, clinicians observe the tics directly, but a formal diagnosis isn’t usually given right away. Because tics are common in childhood and often resolve on their own, the standard approach is to watch and wait. “If the tics are going on for a period of time — say, a couple of months or three to four months — then let’s talk about what we can do to help,” he explains.
That waiting period is actually built into the diagnostic criteria. As mentioned earlier, tic disorders are classified based on the type of tic(s) present and how long symptoms have lasted.
Do tics change over time?
Tics can naturally progress over time, but this is not to say that they worsen. Dr. Piacentini notes that roughly 15-20% of young school-age children experience some tics and that most begin the same way — at the top of the body and moving downward over time.
In those 15-20% of young school-age children who experience tics, the first tics to appear are almost always motor tics, typically facial or head-based. The most common early tics include blinking the eyes, opening the eyes wide, grimacing, squinting, and making minor head movements. From there, tics may progress to the shoulders, then the torso — stomach tensing, for example — and eventually to the arms, hands, and legs.
In addition, vocal tics typically emerge about one to two years after motor tics do — and not every child develops them at all. Early vocal tics tend to be simple: humming, snorting, sniffing, making animal sounds, or uttering isolated syllables. Like motor tics, they can progress from simple to more complex, eventually involving phrases, sentences, or louder sounds.
The vocal tic most associated with Tourette syndrome in popular culture — coprolalia, the involuntary use of profanity or offensive language — is actually quite rare. Dr. Piacentini notes that only about 10-15% of patients experience it, and it is more commonly seen in older patients.
In this video, Dr. Piacentini dives deeper into the progression of tics:
How environment and stress affect tics
The environment plays a big role in the frequency and intensity of tics, something Word knows firsthand. For her, the start and end of the school year — transitions, new routines, added pressure — are when she notices her tics picking up most. Any disruption can inadvertently cause stress, and stress, as it turns out, is one of the most consistent tic triggers.
Studies have found that family-related stress, personal relationship stress, and school-related stress are all independently associated with increased tic severity. One large survey found that nearly 97% of patients reported their tics worsened due to psychosocial (an individual's psychological state and their surrounding social environment) stress or anxiety.
In this video, Word shares more on how stress impacts her Tourette syndrome:
Dr. Piacentini explains why the environment has such a powerful impact on tics.
“Tics are very, very sensitive to the environment,” he says. “If you tell a child not to tic, they’re going to tic. If you create a stressful environment for someone with tics — if they know they’re being watched or scrutinized — they’re going to tic."
He describes Tourette syndrome as a disorder of inhibition, where the brain struggles to suppress unwanted behaviors. When a person feels pressure to hold back a tic, they think about it more and grow more anxious, and that anxiety makes the tic more likely to break through.
When people try to hold back their tics, the effort itself can cause stress, and the tic may actually worsen. For that reason, Dr. Piacentini says the first thing he tells parents is to ignore the tics entirely. Drawing attention to a tic — even with concern — can make a child more self-conscious, more anxious, and more likely to express tics. The goal is to avoid building an association between the tic and negative attention before that pattern takes hold within those first couple of months of tics occurring.
Dr. Piacentini also describes a scenario he sees often: a child comes in with tics, but there’s also a lot of stress at home — tension between parents, conflict, uncertainty about treatment. Even if the tics are the most obvious problem, none of it can be addressed effectively until the environment is stable enough for treatment to take hold. “The parents and family members don’t need to like each other,” he says, “but we need to create an environment that’s going to allow this treatment to work.”
Dr. Piacentini shares more on how the environment impacts Tourette syndrome in this video:
Common co-occurring conditions
According to the Tourette Association of America, an estimated 83% of people with Tourette syndrome have at least one co-occurring condition. The most common include attention deficit/hyperactivity disorder (ADHD), obsessive compulsive disorder or behaviors (OCD/OCB), anxiety, behavioral and emotional challenges, specific learning disabilities, social skills deficits, sensory processing issues, sleep disorders, and functional neurological disorder (FND).
Dr. Piacentini notes that when a child first comes into the clinic, part of the evaluation is ruling out other causes. While tics are almost always the straightforward explanation, he is careful to note that occasionally they can signal something else entirely — another underlying medical condition that deserves attention before a tic disorder diagnosis is confirmed. Below, we’ll dive briefly into two of the most common co-occurring diagnoses that are often seen with Tourette syndrome.
ADHD as a co-occurring diagnosis
Of all the conditions that can accompany Tourette syndrome, ADHD is the most common, as 60–80% of people with Tourette syndrome also have ADHD. When the two occur together, the challenges can multiply quickly. A child who is already working hard to manage tics may also be having difficulty focusing, staying organized, and regulating impulses, and each individual condition can make the other harder to handle.
As parents, you may find yourself unsure of which problem to address first, or you might wonder whether treating one could make the other worse. Dr. Piacentini says this is one of the most common and complicated situations he sees in his clinic, and the answer isn’t always straightforward. “We need to figure out what is the most serious problem or which one is going to interfere with our ability to treat the other(s),” he explains.
In this video, Dr. Piacentini dives deeper into ADHD as a co-occurring diagnosis:
The reason it is so important to determine which diagnosis to treat first is because it impacts the primary behavioral treatment for tics — called Comprehensive Behavioral Intervention for Tics, or CBIT. CBIT requires a child to notice the urge to express a tic before it actually happens and then redirect it. That takes focus, self-awareness, and sustained attention. If ADHD is untreated, those skills are much harder to access. As Dr. Piacentini puts it, “If a child has untreated ADHD, they need to get that treated before they can do CBIT. If [they] have issues with attention, they’re going to struggle to be able to pick up on the urge.”
This is why, in many cases, ADHD gets addressed first, even when the tics seem like the more pressing problem. Treating the symptoms of ADHD can also reduce overall stress and anxiety, which may help lower tic severity as well, so the benefits can work in both directions.
OCD as a co-occurring diagnosis
After ADHD, OCD is the next most common condition to accompany Tourette syndrome. Up to 50% of individuals with Tourette syndrome also experience symptoms of OCD, and for parents, the two can often be difficult to tell apart. (Sometimes it’s even difficult for clinicians to tell them apart.)
To understand why they overlap so much, Dr. Piacentini uses a framework he developed for his own clinic. He describes tics, OCD, anxiety, and/or body-focused behaviors like skin picking and hair pulling as all belonging to the same family of experiences, what he calls disorders of negative reinforcement. This revolves around the idea that when something uncomfortable goes away after you do something, you are more likely to do that thing again. With tics, performing the tic relieves the premonitory urge; that building pressure fades only once the tic happens.
With OCD, completing a ritual makes the anxious thoughts go away.
“If I touch something and I’m afraid I’m going to get contaminated, and I do my ritual, that fear goes away,” Dr. Piacentini explains.
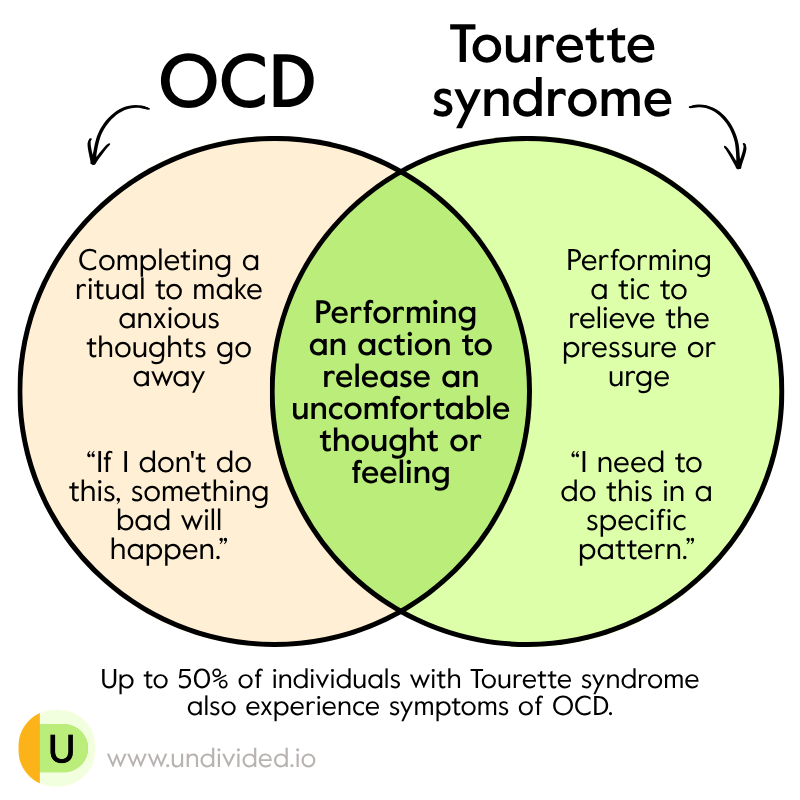
Yet both share the same general principle of performing an action to release an uncomfortable thought or feeling. It is why OCD and tics so often show up in the same child and why the line between them can get so blurry. Dr. Piacentini points to a specific phenomenon called Tourettic OCD, which focuses on the overlap of tic and OCD symptoms.
Unlike typical OCD, which is usually driven by anxiety and obsessional thoughts, such as “if I don’t do this, something bad will happen,” Tourettic OCD is more often driven by a feeling of intense physical discomfort that is briefly alleviated if tics are performed “just right." “It’s not fear-based,” Dr. Piacentini says. “It’s like, ‘I need something to be a certain way. I need to do this in a specific pattern.’” He has worked with children whose OCD tells them they need to snap their fingers three times or repeat a movement in a precise sequence. “There’s a line between tics and OCD,” he says, “but it’s actually very blurry.”
Dr. Piacentini dives deeper into the connection between OCD and Tourette syndrome here:
When OCD and tics are both present, clinicians treat both, but the order depends on the child. Dr. Piacentini’s clinic might spend four weeks on CBIT for tics first, then shift focus to OCD treatment. In cases where the two are hard to separate, the team typically makes a comprehensive list by distinguishing urges, thoughts, and feelings and works through them together. “The order in which we do so really depends on the presentation,” he says.
For parents, the most important takeaway is that OCD in a child with Tourette syndrome may not look like what you expect. It may not be about fear of germs or checking the locks. It may look like a compulsion to do something a certain number of times or an intense need for things to feel “right” before moving on — and that can be easy to miss or misread. That’s why it’s so important to work with your child’s health care professional to help identify and treat both co-occurring diagnoses.
Treatment for Tourette syndrome symptoms
Before diving into specific treatments, Dr. Piacentini offers an important clarification for parents: there is no cure for Tourette syndrome. Treatment for Tourette syndrome can only reduce the impact of tics to a point where a child can function comfortably. “Sometimes the best outcome of treatment is that the child and family learn more about the tics, the school gets educated, and the child is able to manage their tics in most situations — but may tic freely in others,” he explains. The goal is not elimination, but a meaningful improvement to the quality of a child’s life.
Comprehensive Behavioral Intervention for Tics (CBIT)
The first line of treatment recommended by clinicians today is not typically medication but CBIT. For many years, medication was the only real treatment option for children and adults with Tourette syndrome, but researchers working with the Tourette Association of America developed and tested CBIT as a promising non-medication alternative.
CBIT builds on an earlier treatment called Habit Reversal Training, which was developed in the early 1970s. Dr. Piacentini explains that both approaches work by addressing the relationship between the premonitory urge and the tic itself. This type of treatment can be provided by trained health care professionals, such as psychologists, behavioral therapists, occupational therapists, psychiatrists, or social workers who specialize in this type of treatment.
The goal for this treatment is to teach a child to recognize when a tic is about to happen and then to perform a competing behavior. “If I have an urge to tic, I do my competing response instead — I’m going to hold that response for a minute or until the urge goes away,” he says. Over time, this weakens the connection between the urge and the tic.
In Dr. Piacentini’s own study of more than 100 children, more than 50% of participants responded to CBIT, compared to only about 18% who received other forms of treatment. Crucially, when the team followed up with those same children nine years later, they still were benefiting from the CBIT. Meaning, the children who had responded to CBIT still had the same reduced level of tics, while the comparison group had seen their tics return.
CBIT also includes what Dr. Piacentini calls a functional intervention — teaching members of the child’s environment, including parents, teachers, and family members, not to inadvertently reinforce tics by drawing attention to them or calling them out. His personal mantra for this approach:
“Tics — nothing earned from them, nothing lost because of them.”
It is worth noting that some treatments people try for tics don’t always work for them. Dr. Piacentini is direct on this point: while EMDR and neurofeedback are used in clinical settings for other conditions, neither has been scientifically proven for treating tics, and the research does not support their use for this specific purpose.
Word's own experience reflects the importance of finding the right approach. "CBT has helped so much," she says. "That's been by far the most successful. I had one therapist who wanted to experiment with EMDR, and it just didn't click."
Knowing what types of treatments are available is the first step in finding the one that clicks for your child.
Medication
When behavioral therapy alone is not sufficient, antipsychotic medications such as risperidone (Risperdal), haloperidol (Haldol), pimozide (Orap), and aripiprazole (Abilify) may be considered. (Note: this is not medical advice. Please contact your doctor for appropriate advice.) Haloperidol, pimozide, and aripiprazole are currently the only medications approved by the FDA to treat tics. Of these, Dr. Piacentini notes that aripiprazole has the most formal research behind it and is generally better tolerated than older medications like haloperidol.
A second class of medications, the alpha-2 adrenergic agonists, includes Clonidine and Guanfacine. These are often considered a first-line pharmacologic option, and for patients with co-occurring ADHD, they may help reduce tic severity and ADHD symptoms simultaneously. They tend to be somewhat less effective than the antipsychotic medications but appear to have fewer side effects.
In this video, Dr. Piacentini shares more about common medications used to treat Tourette syndrome.
Dr. Piacentini is honest about the trade-offs, though. Antipsychotic medications can cause side effects including drowsiness, weight gain, fatigue, and movement problems such as tremors. He strongly recommends that any medication for tics be managed by a psychiatrist or pediatric neurologist with relevant experience, that it not be started lightly, and that it always be used in conjunction with behavioral therapies (like CBIT) when possible.
“These are pretty powerful medications, and we do our very best not to start treatment with them,” Dr. Piacentini says. “They have a number of side effects, but they can be effective in some cases.”
Deep Brain Stimulation
For the vast majority of people with Tourette syndrome, behavioral therapy and medication are enough to manage symptoms meaningfully. However, for a small number of adults whose tics remain severe and debilitating despite exhausting every available treatment, deep brain stimulation (DBS) can be an option.
Deep brain stimulation is exactly what it sounds like. It works like a pacemaker but for the brain. The procedure involves surgical placement inside the brain of a small electrode that delivers electrical stimulation that blocks the nerve signals responsible for tics. Dr. Piacentini emphasizes that this is typically a last-resort treatment, and a patient must have tried and failed every other identified treatment before it is even on the table.
It is generally accepted that DBS should be reserved for adults, as most cases of Tourette syndrome improve on their own during early adulthood. The procedure is typically offered to people over the age of 20 and is only considered appropriate for those with severe tics that have a significant impact on daily life. It is not a treatment for children.
Although behavioral and medication treatments are available for most patients, DBS has emerged as a potential option for those with severe Tourette syndrome that does not respond to conventional treatments. That said, it still is experimental. The FDA has not approved DBS specifically for Tourette syndrome, though clinical studies have shown it can be used safely and effectively in carefully selected adult patients.
Dr. Piacentini also mentions transcranial magnetic stimulation (TMS) as another emerging treatment being tested, though he notes that for most families reading this, these options are far down the road — and for most children, they will likely never be needed at all.
Setting realistic expectations for treatment
Perhaps most importantly, Dr. Piacentini reminds parents that success in treatment does not mean a child will stop having tics entirely. There is currently no cure for Tourette syndrome, and that distinction matters when defining what a successful treatment actually looks like. “When we talk about treatment working, we mean we reduce the impact of the symptoms in ways that allow the child to function well.”
“The child is going to tic still,” he says, “but people don’t really notice, or the child is able to manage their tics in most situations.” In other words, children can be taught how to live with their tics and potentially lessen them. But, ultimately, there is no current treatment that stops Tourette syndrome.
For Word, that shift in perspective made all the difference.
“I learned that tics don’t need to be stopped,” she says. “It’s just not worth it, physically and mentally, to try to make them stop.”
Therapy and medications help provide support for individuals seeking relief and/or support with Tourette syndrome.
There’s a common misconception that tics are something a child can control — like a switch they can easily flip on and off. This is untrue.
Dr. Piacentini explains that tics happen in the middle of other activities, without warning or planning. “It’s not like a kid says, ‘I’m going to tic now.’” Young children in particular are often completely unaware they are doing it. “They’re just being little kids, playing with [their] blocks, making a noise, and they may not really have that kind of awareness,” he says, which is something he sees regularly in early-onset cases.
In Word’s experience, Tourette syndrome isn’t something that’s easily controllable, and the social pressure that comes with Tourette syndrome never fully goes away.
“I think people assume that it’s always 100%,” she says, “that tics can’t really have a range. But mine do. I have some very mild ones that can go unnoticed in a conversation, and then I’ve got some that refuse to be ignored.”
The fact that children with Tourette syndrome cannot control their tics — or may struggle to do so — is one of the most important things parents and teachers can know. It becomes especially important when one of the most common complaints parents hear from school is that their child is deliberately being disruptive.
One way to distinguish a tic from a deliberate behavior, Dr. Piacentini explains, is to simply ask the child if they are able to stop their tic. A child engaging in volitional (voluntary) behavior — something they are choosing to do — can generally stop when asked. A child with tics may be able to suppress the tic briefly, but it will almost always return, often with greater frequency. Volitional behaviors also tend to have a clear purpose: a child hits something because they are angry, or refuses to go to school because they do not want to be there. Tics, by comparison, are not deliberate and rarely correlate with what a child is thinking or feeling in the moment.
It is worth mentioning that this is meant as a one-time or one-off diagnostic distinction, not a parenting strategy. As Dr. Piacentini emphasized earlier, repeatedly asking a child to stop ticking creates pressure, heightens anxiety, and can actually make tics worse. The goal here is simply to help parents and teachers understand the difference between a tic and a choice, not to use suppression as a management tool.
“I’m blinking my eyes, I’m shaking my head — it’s just kind of out of context with what’s going on,” he says.
That distinction matters — especially in a school setting, where a child’s tics can often be mistaken for acting out, goofing around, or misbehaving.
Attention and focus
One of the most significant barriers to learning is attention. A child who is actively working to suppress a tic is spending mental energy that cannot go toward listening, reading, or processing what a teacher is saying. Not to mention, given that many individuals with Tourette syndrome also have a co-occurring diagnosis of ADHD, attention can be even more difficult.
Vocal tics can also put children in particularly difficult positions at school. A child who blurts out sounds, words, or phrases due to a tic has no control over that behavior, yet it can easily be misread by teachers and staff as deliberate disruption. Children with Tourette syndrome benefit when schools use positive rather than punitive disciplinary strategies. Students should not be disciplined for behaviors that are direct manifestations of their disability, and families advocating for a child in this situation may want to request a Manifestation Determination, a formal process that examines whether a student’s behavior is tied to their disability, before any disciplinary action is taken.
Motor skills and handwriting
Tics can also interfere directly with physical tasks. The vast majority of students with Tourette syndrome may experience difficulty with written language, for a wide variety of reasons. Tics affecting the hands, fingers, wrists, arms, shoulders, or eyes can make handwriting difficult, and a child may write very little or resist writing altogether.
Margins and spacing may also be inconsistent, and a student’s handwriting might look neat one day and fall apart on a longer assignment the next. Extra practice or rewriting typically does not lead to improvement when tics are the underlying cause.
Language and echolalia
Some children with Tourette syndrome also experience echolalia, the involuntary repetition of words or phrases they have just heard. Echolalia occurs in many cases of Tourette syndrome, and the repetitions are mainly repeating their own vocal tics. It is worth noting that echolalia is not exclusive to Tourette syndrome; it has also been described in autism, ADHD, aphasia, and several other neurological and developmental conditions, and it is actually a part of language development in toddlers.
Children use echolalia as they learn how to communicate, but it may also be a sign of developmental delay or an underlying condition if it continues or appears during adulthood.
Related to echolalia is gestalt language processing, a style in which a child acquires language in whole chunks or phrases rather than word by word. Gestalt language processors absorb language they hear and store it as a whole unit, later using those phrases to communicate, sometimes in ways that can seem out of context to those around them. Echolalia can be described as either immediate or delayed, and marks the first stage in the gestalt language processing framework of language development. Read our Gestalt Language Processing (GLP) 101 article to learn more.
Social functioning, friendships, and bullying
Lack of social acceptability, deficits in social self-esteem, and difficulty establishing and maintaining friendships are commonly found in children with Tourette syndrome during clinical evaluations. Middle school tends to be the hardest period for everyone, but especially for students with Tourette syndrome. Children with Tourette syndrome are particularly vulnerable to being teased or excluded by peers because of noticeable tics, which over time can limit opportunities to develop social skills and friendships.
Word remembers that period vividly. “When you're 12 or 13, you already feel kind of alien," she says. “Adding insult to injury and realizing there was something neurological that made me not able to control my face was really, really hard." She found herself making jokes at her own expense just to get ahead of other people's reactions.
“I was putting myself down to try and seem normal. Once I stopped doing that, I realized there's nothing actually wrong with having Tourette's."
One of the most important proactive factors is having even one close friend who understands. A stable friendship can moderate the negative effects of social exclusion and even buffer the consequences of bullying. For parents, fostering those connections — through sports, after-school programs, or community activities built around shared interests — is worth actively prioritizing. And for any child still in the thick of it, Word offers this: “When you find good people, they're not going to care. It's just a part of you — it isn't you."
School supports for Tourette syndrome
For students with Tourette syndrome, school can be one of the most challenging environments to navigate. The good news is that there are formal protections and supports available — parents just need to know what to ask for.
Understanding how Tourette syndrome is classified
Tourette syndrome is recognized under the Individuals with Disabilities Education Act (IDEA) as “Other Health Impairment (OHI),” a classification that matters more than it might seem. As the Tourette Association of America has noted, Tourette syndrome is commonly misunderstood to be a behavioral or emotional condition rather than a neurological one, and including it explicitly under this definition is meant to help correct that misperception and prevent the misidentification of students’ needs. In other words, a child with Tourette syndrome should not be treated as a discipline problem. Their tics are symptoms of a neurological condition, not deliberate actions.
IEP vs. 504: What’s the difference and which does your child need?
Mary Peitso, a special education advocate with more than two decades of experience representing families across California, explains that a Tourette syndrome diagnosis can qualify a child for a 504 plan but not necessarily an IEP. The distinction comes down to impact. Peitso explains that in order to qualify for an IEP parents must be able to demonstrate how Tourette syndrome impacts your child's ability to learn.
A 504 plan details the accommodations and modifications a student needs in order to have equal access to education. An IEP contains those same accommodations and modifications but typically goes a step further, detailing and/or offering more the individualized supports and services to be provided. Think of it this way: a 504 plan provides primarily accommodations, while an IEP adds services and goals on top of that.
To demonstrate that Tourette syndrome is adversely affecting your child’s education, Peitso recommends requesting a psychoeducational evaluation from the school district. “That will probably show a pattern of strengths and weaknesses and deficits in some areas — possibly academic, but more so socially, emotionally, and behaviorally,” she explains. If parents disagree with the district’s findings, they have the right to request an independent evaluation at public expense.
A child can also start with a 504 plan and transition to an IEP if their needs increase over time. When that happens, Peitso notes, the accommodations already in the 504 plan typically get written directly into the IEP.
What services for Tourette syndrome are included in an IEP?
The services built into an IEP depend on the individual child, but Peitso commonly sees counseling services, social skills training, and Resource Support Program (RSP) services for students whose grades are being affected. RSP services — provided by a credentialed special education teacher — can be delivered either inside or outside the classroom and are designed to support students in the academic areas where they are struggling.
If a child needs counseling or social skills support, those services require an IEP rather than a 504 plan. Peitso explains, “504 plans typically only have accommodations."
Common 504 and IEP accommodations for students with Tourette syndrome
Because not every child with Tourette syndrome has the same symptoms, supports must be tailored to their specific needs. That said, Peitso points to several accommodations she sees most often — and offers some important guidance on how they should be written.
Common 504/IEP accommodations:
Extended time for completing classwork, tests, homework, etc.
Breaks after prolonged cognitive demands
No late penalty for schoolwork
Noise-canceling headphones to avoid overstimulation
Ability to go to a space where they can tic without being observed
Visual schedules and checklists
Flexibility with attendance and tardiness
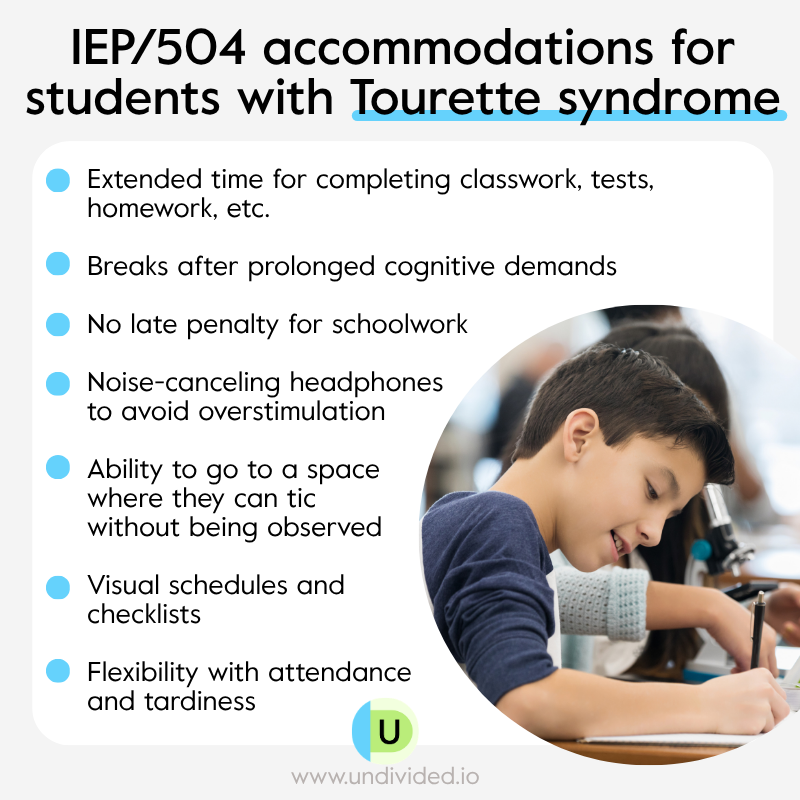
Extended time is one of the most common accommodations, but Peitso cautions against vague language. “I frequently see it written as ‘extra time as needed,’” she says. “It’s always needed, or it wouldn’t be in the IEP.” She recommends being specific: extra time on tests, extra time completing homework, up to two weeks with no late penalty, and so on.
The same principle applies to breaks. Instead of “breaks as necessary,” she recommends language like “breaks after prolonged cognitive demands” — for example, after sitting through a 30-minute lecture or test. Other accommodations she recommends include a private space where a child can tic without being observed, noise-canceling headphones for overstimulating environments, visual schedules and checklists to help students who lose their place when they tic, reduced visual clutter in the classroom, and flexibility with attendance and tardiness for students whose tic severity fluctuates day to day. “No parent should get a truancy notice for disability-related behavior,” she says.
In this video, Peitso shares some more accommodation for students with Tourette Syndrome:
For students whose tics involve spitting or other socially disruptive behaviors, accommodations can be tailored accordingly. Peitso gives the example of providing a box of tissues and writing into the plan that when a student feels the urge to spit, they will use a tissue instead. For students with vocal tics, having a designated space to go and release those tics — without judgment or punishment — can make a big difference.
Staff training and awareness
One of the most important accommodations is staff training, and Peitso says it can and should be written directly into the IEP. “You get yard duty monitors who just don’t get it, and kids are getting in trouble all the time for something they can’t help,” she says. The more staff understand about Tourette syndrome — not just that tics exist, but how they affect a child neurologically in real time — the better equipped they are to respond appropriately.
Peitso also recommends that parents document everything. “If it’s not in writing, it didn’t happen,” she says. If your child is being disciplined for tic-related behavior, communicate directly with the principal and teacher, follow up every phone call with an email summarizing the conversation, and share as much information about Tourette syndrome as possible. Some parents, she notes, have gone into schools themselves to lead staff trainings. Some students have done the same — presenting to their classmates about their diagnosis — and found that it helped to reduce the stigma that often comes with Tourette syndrome, which helped to stop the bullying before it started.
Self-advocacy and peer support
Educating a student about their own symptoms is important for self-esteem; their ability to explain their experience to others is also an important form of self-advocacy. Word expressed that learning to walk up to a teacher and say clearly and confidently, “I have Tourette syndrome, this is how it affects me, and this is what I need,” wasn’t easy, but it changed her school experience entirely.
“The default was apologizing,” she says. “But I got sick of that. This is something I need, and I should be able to communicate what I need to succeed as a student without having to apologize for it.”
Peitso echoes that sentiment, noting that accommodations work best when students know they have them and feel empowered to use them on their own terms. “It’s better to have it in the IEP and have the student learn to self-advocate,” she says. And her parting advice for any parent navigating this process for the first time? “Don’t be afraid to be a squeaky wheel — but be a nice squeaky wheel.”
Common myths about Tourette syndrome
At the 2026 BAFTAs, a Tourette syndrome advocate whose life inspired the film I Swear involuntarily shouted a racial slur during a speech. The moment went viral almost immediately, and he faced heated backlash that started a public debate about Tourette syndrome and its most misunderstood symptoms — the assumption that people with Tourette syndrome can control what they say, or that because they said it, they must have meant it.
For the Tourette community, the reaction was painfully familiar. Word had seen it coming. “There’s always stuff in the news like that,” she says. “It was just a huge misunderstanding that society perpetuated into something crazy.” The BAFTA incident pulled into sharp focus just how much the general public still misunderstands Tourette syndrome — and how much damage those misunderstandings can cause. To help dispel some of those misconceptions, we’re busting some of the more common myths below!
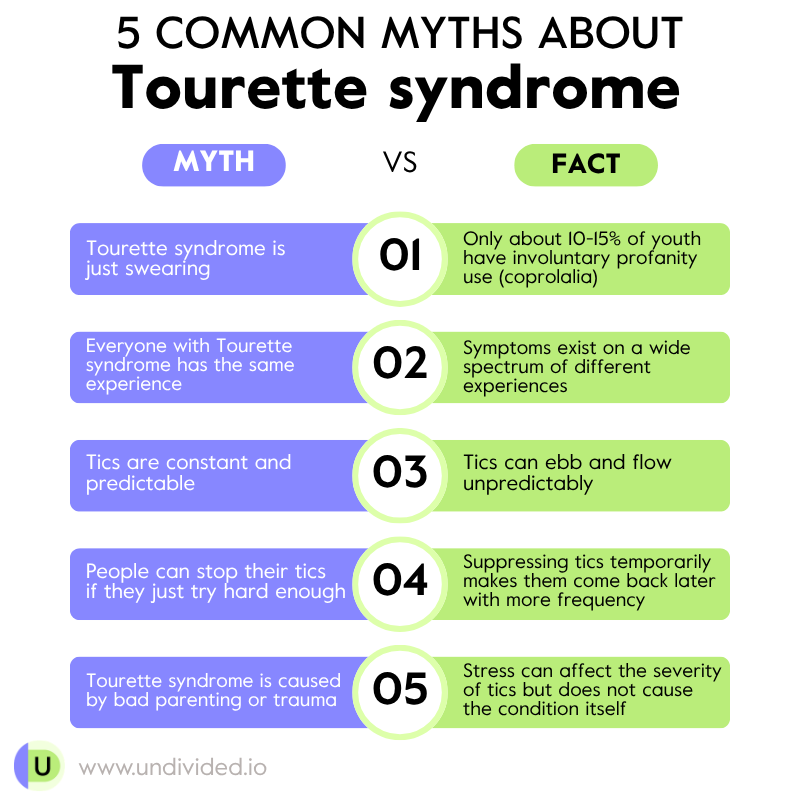
Myth: Tourette syndrome is just swearing
This is by far the most persistent myth, and it is fueled almost entirely by how Tourette syndrome is portrayed in movies, television, and viral moments like the one at the BAFTAs. Dr. Piacentini is direct about it. The involuntary use of profanity or offensive language is called coprolalia, and it is actually quite rare. “Only about 10–15% of youth have coprolalia,” he says. “But, we see that condition more on TV and in the movies because it’s flashy.”
In this video, Dr. Piacentini explains further about coprolalia and Tourette syndrome:
Coprolalia seems to have become the defining image of what Tourette syndrome is. Word finds this deeply frustrating. “Whenever I tell somebody I have Tourette’s, the first thing is always about the cussing,” she says. “Mine aren’t that cool. I don’t get to do that.”
Myth: everyone with Tourette syndrome has the same experience
Tourette syndrome exists on a spectrum, and no two people experience it the same way. Word pushes back on the assumption that her experience is somehow less valid because her tics are not the kind that demand a room’s attention. “Just because I don’t have the specific tic where I’m shouting or cursing doesn’t mean I have an easier form of Tourette’s,” she says. “I think people always assume it’s the most extreme version of everything, and that assumption ends up hurting me — because people assume I can’t be calm or in quiet situations.”
In this video, Word touches more on the range of Tourette syndrome:
Myth: tics are constant and predictable
One of the most confusing aspects of Tourette syndrome for those unfamiliar with it is its unpredictability. Tics ebb and flow, and a child can have an entirely tic-free day followed by a very difficult one with no clear explanation. “There will be times where I wake up and I’m having a really bad tic day, and I don’t know why,” Word says. “Nothing happened, nothing freaked me out. It just happens sometimes. It’s like sneezing for me.” She wishes more people — teachers, peers, and even well-meaning adults — understood this. “I need a little more grace from people when days like that happen. I don’t know why it happens. It just does.”
Myth: people with Tourette syndrome can stop if they just try hard enough
This is one of the most damaging misconceptions because it places the burden of an involuntary neurological condition on the person experiencing it. Dr. Piacentini explains that while a child may be able to suppress a tic briefly when asked, it will almost always return — often with greater frequency. The effort of holding a tic back does not make it go away, but simply delays it. The exception to this is behavior therapy, e.g., CBIT, where the child can learn to manage their urges to tic which then can lead to a reduction in the frequency and/or severity of tics.
Word knows this better than anyone because for years she masked her tics at school, physically covering her face and hiding herself to keep her tics from being seen. “It takes a lot of effort,” she says.
“Sometimes it hurts, because I’m holding back so much. It’s like every single muscle in your body is tensed up at once, and it won’t release until you get home.”
What Word is referring to is masking, a social coping strategy that involves hiding their differences (or symptoms of their disability) in order to manage social situations and fit in with others. Masking can include actions like suppressing stimming behaviors, such as flapping of hands, adjusting face and body to appear more relaxed or confident, hiding discomfort, forcing smiles or excitement when you naturally have a flatter affect, and forcing eye contact.
The cost of masking is often very real and physical. Word explained that she would often come home exhausted, get headaches, and need to lie down. Her mother thought she had mono because of how much she was sleeping.
Eventually, Word reached a breaking point. “I got sick of having to hide for the courtesy of others,” she says. “It’s just not worth it in the end, because people would still say things.” The expectation that someone with Tourette syndrome should simply mask their tics all the time is unrealistic.
In this video, learn more about what Tourette syndrome looks like for Word:
Learn more about masking in our What Is Masking? article.
Myth: Tourette syndrome is caused by bad parenting or trauma
When a child is first diagnosed, one of the most common reactions from parents is guilt. They search back through their child’s life, looking for something they did wrong — a period of too much stress, a move, a difficult year — convinced that something in the environment they created must have triggered it. Word’s parents were no different. “My parents were worried that they did something,” she says. “That they pushed me too far, or I was way too stressed out, and then it immediately happened.”
Dr. Piacentini explains that this is not how Tourette syndrome works. The exact cause of Tourette syndrome is not fully understood, but it is believed to involve a combination of genetic and environmental factors, as well as brain structure and function. It is not the result of parenting choices, trauma, or stress. Those things can affect the frequency and severity of tics, as discussed earlier, but they do not cause the condition itself.
Word’s message to parents carrying that guilt is simple:
“There’s nobody to blame for it. It’s just something that happened. It was just the luck of the draw.”
The most productive thing a parent can do, she says, is to not look backward for a cause, but look forward and focus on making sure their child feels comfortable, seen, and anything but abnormal.
Key takeaway for parents: supporting your child with Tourette syndrome
Perhaps the most important thing a parent can do for a child with Tourette syndrome is what Word’s parents did for her: tell their child, early and often, that there is nothing wrong with them. That this is simply the way their brain works. That they are not broken, not weird, not less deserving of a seat at the table than anyone else. Word remembers her parents helping her through her hardest years, reminding her that things would not always feel this overwhelming. “A parent’s job,” she says, “is to bring their kid down off that ledge.”
She speaks from experience when she says it gets better. The tics that felt all-consuming at 13 have become, at 19, simply a part of who she is. Her friends do not baby her. Her teachers supported her. Word has learned to advocate for herself, to shut down ignorant questions with confidence, and to stop apologizing for something that was never her fault to begin with.
“Just ride the wave,” she says. “It will get better. You will not feel like this forever. You just have to give yourself grace and realize, ‘I’m going to grow into this. It’s going to happen.’”
And for the parents reading this who are still in the thick of it, still trying to figure out what their child needs and how to fight for them, you being here is a sign that you are already doing the right things. Keep going! Ride the wave and make sure your child knows they are seen, they are supported, and they are going to be okay (and you will be too).




Unlock more with Undivided
Turn knowledge into action that benefits your child
Get Membership




Author

